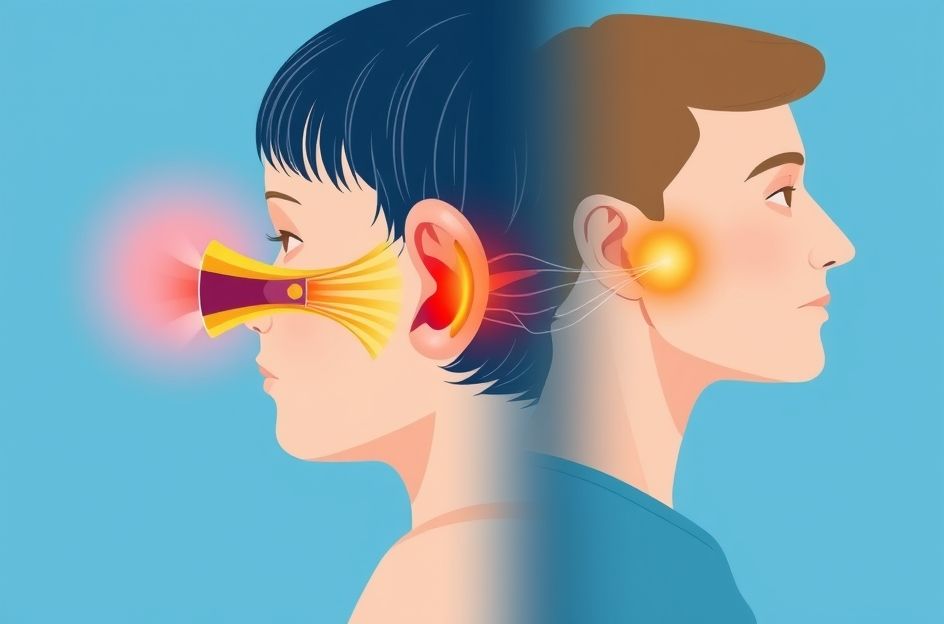
Otitis media, an inflammation of the middle ear, often involves fluid accumulation that can become infected, leading to otitis media with effusion (OME). In many allergic rhinitis patients, chronic OME stems from IgE-mediated allergies. This type of allergy occurs when IgE antibodies, produced by plasma cells in response to foreign substances entering through the nasal mucosa, bind to mast cells. This binding triggers the release of histamine, a chemical that causes nasal itching and hypersensitivity.
Research indicates a strong correlation between allergic rhinitis and OME. One study revealed that 50% of children with chronic OME also had nasal allergies. Studies have also examined the impact of seasonal allergic rhinitis on Eustachian tube function and middle ear pressure. Pollen exposure can increase Eustachian tube obstruction from 15% to 60% in pollen-allergic individuals. Exposure to ragweed pollen, a seasonal allergen, elicits immune responses in both the Eustachian tube and nose. Similarly, perennial allergens like house-dust mites can also cause Eustachian tube obstruction; one study found that 55% of adults with nasal allergies experienced Eustachian tube dysfunction upon exposure to house-dust mites.
Further research highlights the frequent occurrence of Eustachian tube obstruction in allergic rhinitis patients, with nasal obstruction often preceding Eustachian tube issues. Allergen provocation studies have detected inflammatory mediators like histamine in the middle ear effusions of children with OME. Untreated Eustachian tube obstruction, particularly from perennial allergens like house-dust mites, can lead to middle ear disease, especially when priming occurs. Priming refers to the mucosa’s heightened response to even low doses of allergens upon repeated exposure. Allergic rhinitis exhibits similar priming effects, where the nasal passage becomes hyperresponsive to inhaled allergens. Physiologic hyperresponsiveness from seasonal allergens like ragweed pollen can persist beyond the pollen season.
Viral upper respiratory tract infections (URTIs) are also implicated in otitis media, with approximately half of new cases diagnosed shortly after a viral infection. While traditional culture techniques rarely isolate viruses from middle ear effusions, PCR-based molecular analysis has detected viruses in 53% of middle ear effusions. Experiments involving rhinovirus-39 infection demonstrated increased Eustachian tube dysfunction and abnormal middle ear pressure in about 30% of participants, although they were less likely to develop otitis media. Intranasal inoculation with influenza A virus led to middle ear under pressure in 59% of participants, with 25% developing otitis media. In one instance, a patient developed middle ear under pressure followed by purulent otitis media, with PCR analysis confirming the presence of both influenza A and Streptococcus pneumoniae. Viral infections contribute to Eustachian tube dysfunction and abnormal middle ear pressure, predisposing individuals to otitis media.
Recent studies of children with acute otitis media found that 65% of middle ear fluid samples contained both bacteria and viruses, suggesting that viral infections create a favorable environment for bacterial growth.
In conclusion, allergic rhinitis and common colds/flu can trigger Eustachian tube obstruction and middle ear pressure imbalances, potentially leading to OME and permanent hearing impairment. Prompt treatment of allergic rhinitis and URTIs is crucial to prevent the development of chronic sinusitis and OME, which can be challenging to treat.